




Images and text Genevieve Carbonatto
It is a busy Thursday evening in the Emergency Department. There is no place to put patients and assess them. The only bay which may be available is occupied by a lady who refuses to leave the bay because she feels so ill. You call the nurses and together you create a bed where this lady can lie down in – not an easy task. The next patient to be seen has been waiting 2 hours. She is a 34 year old who is 6 weeks pregnant and has had acute onset abdominal pain ealier that day (around 2.00pm) . She is sitting comfortably with her husband in the waiting area. Briefly her story is the following: earlier that week she presented “after hours” to another Emergency Department because of abdominal pain. She had a point of care ultrasound which showed an empty uterus (no intrauterine gestational sac) and no fluid in the pouch of Douglas. She was referred for a formal scan the next day which again confirmed that she had a pregnancy of unknown location and it was organised for her to have a repeat ultrasound in a week with repeat BHCG.
Her BP is 110/70, HR 87/min. Her abdomen is soft but she is uncomfortable suprapubically.
This is a transverse sweep through her pelvis
The uterus is difficult to distinguish and there is a heterogeneous complex mass anterior to the uterus. This is a large heterogeneous echoic blood clot which is interfering with the outline of the uterus.

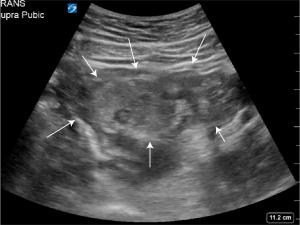
Scanning in the transverse plane does not improve the visualisation of the uterus
Free anechoic fluid in the pouch of douglas is difficult to see. The pouch of Douglas is in fact filled with clotted blood. Scanning through the LIF , free anechoic fluid is clearly visible.
A quick scan of the RUQ shows free fluid in Morison’s pouch
The patient is immediately transferred to the rescusitation bay. The Gyne team are called and she is transferred within the hour to theatre for removal of a left ruptured ectopic pregancy
Teaching point: This case highlights again that severe pain and shock are not always associated with rupture of an ectopic pregnancy. If the examination of the pelvis is difficult using ultrasound, and you are unable to properly see the outline of the uterus on transabdominal scanning consider the possibility of a ruptured ectopic where blood has coagulated obscuring the uterus. Make sure you scan both iliac fossas and scan Morison’s pouch to look for fluid.