



- The EFAST examination is easily achieved in most circumstances. Name 4 clinical situations which may limit the feasibility of the EFAST exam
4 limitations of the EFAST exam
- Morbid obesity – It is very difficult to get good penetration of ultrasound waves through morbidly obese patients which is a significant limitations when performing the exam
- Subcutaneous emphysema – It is not possible to insonate through subcutaneous emphysema.
- It may be difficult to determine whether free fluid is ascites or blood
Some ways of distinguishing between the free fluid and ascitic fluid is through
- Past history (chronic liver disease/malignancy)
- Identifying nodular cirrhosis of the liver. The liver may also be contracted and hyperechoic suggesting chronic liver disease
4. US is not as reliable as CT in identifying solid organ injury
2. There are some technical difficulties with the FAST exam. Most clinicians have little difficulty in locating Morison’s pouch but have greater difficulty in locating the spleen. What is the main cause of non identification of the spleen when insonating the LUQ?
The most common technical error for not being able to identify the spleen is not placing the transducer posterior and superior enough.
The transducer is placed in the posterior axillary line (knuckles against the bed) at the 8th – 9th intercostal space. If the spleen is not visible the transducer is then slid down in that same plane towards the feet slowly until the spleen is identified.
3. Visualising the pericardium may be technically challenging when doing the FAST exam. What are some techniques that can be used to improve visualisation of the heart using the subcostal view?
To identify the pericardium
- Place the transducer as close to the xyphisternum as possible
- Depress the transducer towards the spine and flatten the probe. You may need to use some considerable pressure in some cases
- Get the patient to breath in – this will lower the heart
- Make sure you have enough depth on the screen
- Slide the transducer to the right of the epigastrium so that you are insonating through the liver to visualise the heart
4. Name 3 false positives when identifying free fluid in the RUQ
In the RUQ , fluid in the gallbladder, duodenum, hepatic flexure of the colon or other regions of the bowel and the inferior vena cava can be mistaken for free fluid.
- The gallbladder. When the gall bladder is long and thin and close to the border of the liver it may be mistaken for free fluid. It can be differentiated from free fluid because the gallbladder has more rounded borders. Fanning through the area will also expose the gallbladder as a distinct entity
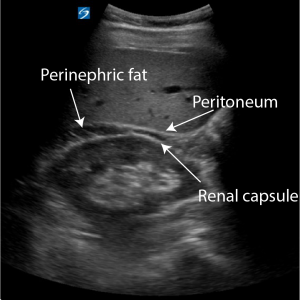
- Perinephric fat. Perinephric fat can appear hypoechoic and sometimes even anechoic. It is differentiated from free fluid because it lies between 2 hyperechoic layers – the peritoneum and the fascia surrounding the kidney

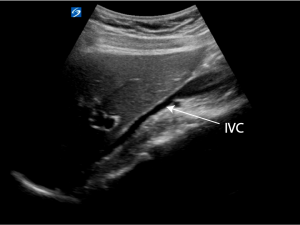
3. The inferior vena cava. The IVC has a hyperechoic border compared to free intra abdominal fluid. Free fluid is also stellate in appearance or has sharper borders than the IVC

Reference
Ma and Mateer’s Emergency Ultrasound (third edition)