



Most answers for this quiz are from the ASE chamber quantification guidelines document 2018
1. What are you looking for when you are eye balling the LV to assess ejection fraction?
Look at
Inward motion of the endocardium
The thickening of the myocardium
The longitudinal motion of the mitral annulus
The geometry of the ventricle
Disadvantage is that it requires a certain amount of experience
The gestalt estimation of cardiac function has been shown to correlate well with actual EF measurements,1 and emergency physicians can visually estimate EF nearly as well as cardiologists.
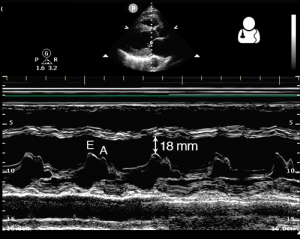
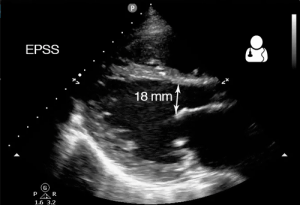
2. What is E- point separation?
There are multiple ways to calculate an ejection fraction, from the simple approximation of fractional shortening to the most accurate (yet cumbersome to calculate) method of discs.
One simple method to estimate EF is to measure the distance from the mitral valve to the septum in mid diastole. This is known as the E-point Septal Separation (EPSS), which correlates well with the EF in a structurally normal heart.
An EPSS < 7 mm is considered normal, while EPSS > 10 mm suggests a low EF. This measurement can be made more accurately when M-mode is used across the tip of the mitral valve in the PLAX view.
Remember that significant mitral stenosis or aortic insufficiency can falsely increase the EPSS measurement, lowering your estimation of the patient’s ejection fraction.
reference : Core ultrasound https://www.coreultrasound.com/uotw-7-answer/
3. At what part of the cardiac cycle do measurements need to be taken to measure global systolic function using linear measurements to measure fractional shortening?
Fractional shortening
-
- Measures the “squeeze “ of the LV .
- Using M mode measure the end diastolic diameter and the end systolic diameter of the left ventricle in the PLAX view or the PSAX view
- Can measure LVEDD and LVESD using M mode or calipers
Linear internal measurements of theLV should be acquired in the parasternal long-axis view carefully obtained perpendicular to the LV long axis, and measured at the level of the mitral valve leaflet tips. Electronic calipers should be positioned on the interface between myocardial wall and cavity and the interface between wall
and pericardium (orange arrows).


Advantages of M mode
- Reproducible
- High temporal resolution
- Wealth of published data
Disadvantages of M mode
- Beam orientation frequently off axis
- Single dimension, i.e., representative only in normally shaped ventricles
Advantage of 2D measurements
- Facilitates orientation perpendicular to the ventricular long axis
Disadvantage of 2D measurements
- Lower frame rates than M-mode
- Single dimension, i.e.,representative only in normally shaped ventricles
2. What are the problems with deriving systolic function using linear measurements?
- M mode cursor has to be exactly perpendicular to the myocardium and at the tip of the mitral valves to be accurate. Improved if using calipers
- It measures myocardial function in one plane only
It is inaccurate if there is
- Conduction abnormalities LBBB or dyssynchrony causing abnormal septal motion
- regional wall abnormalities
- poor image quality and the endocardium is not well visualised
3. What is the normal size of the left ventricle ?
The size of the LV is dependent on sex and body surface area
For males it may vary from 50mm +/- 4 mm in women 45 mm +/- 4mm
4. What is the normal wall thickness of the left ventricle?
Male : normal range 0.6 -1.0 cm , mildly abnormal 1.1 – 1.3 cm, moderately abnormal 1.4 – 1.6 cm , severely abnormal > 1.6 cm
Females : normal range 0.6 -0.9 cm, mildly abnormal 1.0 – 1.2, moderately abnormal 1.3 -1.5 cm , severely abnormal > 1.5 cm
5. What is MAPSE?
MAPSE is the Mitral annular plane systolic excusion
It measures the lateral mitral annular movement towards the apex using M mode.
It is easy to aquire.
A normal MAPSE is > 8mm.
Disadvantages
The lateral mitral annulus needs to move in the same plane as the M mode cursor.
It only represents longitudinal contraction of the left ventricle
6. What is normal Ejection Fraction?
Normal values for LV chamber dimensions (linear), volumes and ejection fraction vary by gender.
A normal ejection fraction is 53-73% (52-72% for men, 54-74% for women).
7. How can you measure Ejection Fraction ?
There are 2 ways of measuring the Ejection Fraction
- Fractional Shortening using Teichholz method. This is what we do in the Emergency Department as a quick and dirty way of measuring ejection fraction. It is however only useful if there are no regional wall abnormalities or conduction abnormalities otherwise it will be inaccurate.
- Simpson’s method
Involves tracing the endocardial border of the LV in the Apical 4 C and the Apical 2C view (Biplane method)
Currently the only method recommended for calculating LV volumes and EF using 2D ECHO.
Disadvantages of the Simpson’s method:
- Takes time to do,
- Need to get good windows with good endocardial wall definition to enable accurate tracing of the endocardial borders.
Inaccurate if there is
- dyssynchrony as it is difficult to define end-systolic and end diastolic frames beat to beat variations such as in atrial fibrillation.
Modified Simpson’s
- Measured from the apical 4- and 2-chamber views (preferably an LV focused view) tracing the endocardial – blood pool interface (between the compacted myocardium and the cavity) at end-diastole and end-systole on images with clear endocardial border definition.
- Papillary muscles should be excluded from the cavity tracing.
- Maximize LV area and avoid foreshortening.
- When approaching the MV plane, the contour is closed by connecting the two opposite sections of the MV ring with a straight line.
- The LV length is the bisector between this line and the apical point of the LV contour distant from it.

8. Name the segments of the left ventricle (1 to 5) below



- apical wall
- lateral wall
- septal wall
- anterior wall
- inferior wall
References
- Ann Card Anaesth. 2016 Oct; 19(Suppl 1): S26–S34 Left ventricular global systolic function assessment by echocardiography Suresh Chengode
- THE AMERICAN SOCIETY OF ECHOCARDIOGRAPHY RECOMMENDATIONS FOR CARDIAC CHAMBER QUANTIFICATION IN ADULTS: A QUICK REFERENCE GUIDE FROM THE ASE WORKFLOW AND LAB MANAGEMENT TASK FORCE https://asecho.org/wp-content/uploads/2018/08/WFTF-Chamber-Quantification-Summary-Doc-Final-July-18.pdf
- http://echocardiographer.org/Calculators/Calculator.COandSV.html