



Images and text Genevieve Carbonatto
A 32 year old lady presents with PV spotting. She is thought to be 8 weeks pregnant. A point of care transabdominal scan is performed in the Emergency Department.
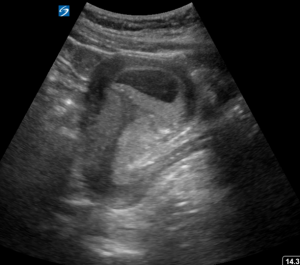
This is her transverse scan of the pelvis
The bladder is empty. There appears to be no gestational sac
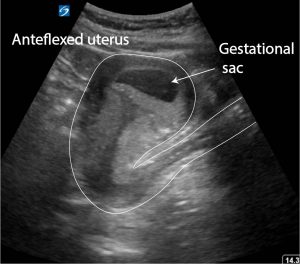
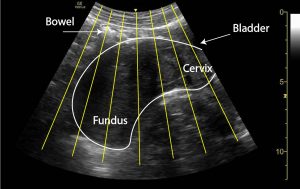
This is her longitudinal scan
The uterus is retroverted. In fact it is retroflexed. A gestational sac is just visible in the fundus but is somewhat hidden by the dirty shadow from overlying gas. Because it is close to the margin of the uterus in this scan, edge shadowing also makes it hard to see.
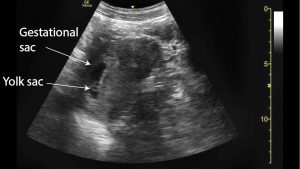
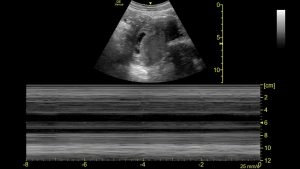
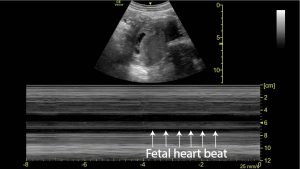
To image the gestational sac better the transducer is slid to the left of the patient in the longitudinal plane and the beam is angled back towards the uterus. Firm pressure is applied to displace the bowel. The yolk sac, the fetal pole and the fetal heart beat can be evaluated.

Discussion
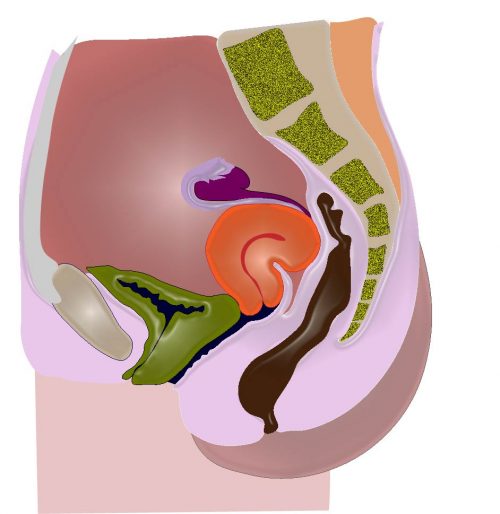
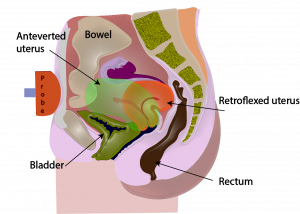
The position of uterus can be highly variable. Most women will have an anteverted uterus but up to 20% of nulliparous women have a retroverted uterus.
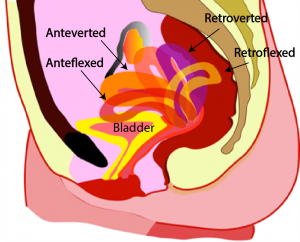
There is usually little problem in imaging the uterus with a transabdominal scan if it is anteverted or anteflexed, even if the bladder is not full. This is because the fundus is close to the probe. The fundus is also perpendicular to the ultrasound beam in this position.
In a retroverted uterus or retroflexed uterus the uterus is bent backwards so that the cervix is tilted upwards with respect to the vagina. The fundus is more posterior than the cervix. The fundus is much harder to visualise in a retroverted or retroflexed uterus because the fundus is much deeper, and the bowel is in the way if the bladder is not full. The ultrasound beam is also travelling more parallel to the uterus which means there is drop out of echoes.
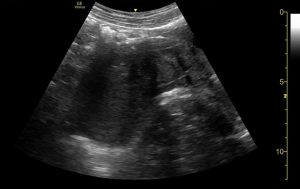
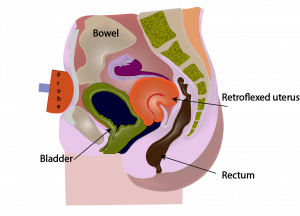
To improve visualisation of a retroverted or retroflexed uterus it is best to wait for the bladder to fill. Otherwise by moving the probe laterally, away from the midline of the uterus and aiming the beam towards the uterus, the fundus is better visualised. Below the first image shows the situation when the bladder is empty and the second when the bladder is full. The bladder is used as an acoustic window.
Teaching point: Be aware that transabdominal ultrasound is not as good as transvaginal ultrasound when evaluating a patient for the presence of a gestational sac in a retroverted or retroflexed uterus. Try these 3 maneuvers first: 1. move away from the midline and look back at the uterus, 2. put firm pressure on the abdomen to move bowel out of the way, 3. re scan when the bladder is full.
During transabdominal gynaecological sonography with adequately filled bladder if we cannot visualise the fundus of uterus then can we label it as retroverted uterus.?
Hello DrIrshad ul haq, I wouldn’t do that. I would state that the uterus was inadequately visualised. There may be another cause for not seeing the uterus – a mass in the way, air from a perforated viscus. It is best to always write just what you see