




Images Genevieve Carbonatto, text Genevieve Carbonatto
An 80 year old lady presents to the Emergency Department with a 4 month history of feeling unwell on and off associated with a 4 kg weight loss during that time. She presented acutely because the night before she developed mild abdominal pain and vomiting. She has been investigated by her GP. Her GP had noted a left upper quadrant mass 6 weeks prior to presenting to the ED. This was thought to be related to the spleen. An urgent ultrasound as an outpatient was reported as normal – no abdominal pathology was identified.
On arrival she is well and triaged category 4. She is no longer nauseous and has no abdominal pain. She has, on examination, a left upper quadrant mass which clinically appears to be her spleen ? splenomegaly. Her bloods were unremarkable.
A focussed point of care ultrasound was performed.
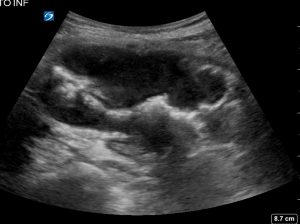
The following is a longitudinal view on ultrasound over the palpable, non tender left upper quadrant mass. The mass is bowel. There is no peristalsis. This patient has a colo colic intussusception. A hypoechoic oval structure is visible with a central hyperechoic region, reminiscent of a kidney. This is the pseudokidney sign. The fat containing mesentery is the hyperechoic centre as the mesentery is telescoped along with the bowel. The hypoechoic oedematous bowel surrounds the mesentery.
.

The pseudokidney sign is present in intussusception but not specific for intussusception. It is found in other bowel pathology such as lymphoma, carcinoma, inflammatory colitis such as Crohn’s disease, ulcerative colitis, infectious colitis. In these situations the hypo echoic area is the oedematous bowel with the apposed mucosal centre the hyperechoic stripe.
This is another longitudinal section of the intussusception. This has been referred to as the hayfork sign.


This is a transverse view of the intussusception. Below is the “doughnut sign”, where in transverse, the intussusceptum ( portion of bowel being dragged or “telescoped” into the adjacent bowel) is visualised within the intussuscipiens (portion of bowel receiving the telescoping bowel)

![]()
The CT confirmed an intussusception of the transverse colon

The patient was taken to theatre and had a subtotal colectomy. At no point prior to her surgery did she feel unwell or develop abdominal pain nausea or vomiting.
Discussion
Adult intussusception is rare. Most intussusceptions in adults are due to a lead point and the most common lead point in adults is adenocarcinoma. This patient did have an adenocarcinoma which was the cause of her intussusception. The interesting part of the story is that a mass had been palpable 6 weeks prior to presenting to the ED so it is possible, if not probable, that this intussusception had been present for at least 6 weeks.
The following are some points about adult intussusception (1,2,3,4)
- In adults it is rare : 1 – 5% of all bowel obstructions
- In adults 70 -90% are associated with a lead point, usually adenocarcinomas (66%) , metastases, polyps, benign neoplasms & lipomas
- Idiopathic intussusceptions in adults are usually due to inflammatory bowel disease, postoperative adhesions or strictures
- In children – it is the opposite 90% of intussusceptions are idiopathic and not associated with a lead point.
- In children symptoms are usually acute associated with abdominal pain, a tender abdominal mass and red current jelly stool.
- In adults symptoms may be acute, subacute or chronic therefore the diagnosis may be missed or delayed.
- Most adults will present with chronic symptoms of partial obstruction.
- In adults the most common presenting symptoms include : Pain (90%) , nausea and vomiting (36 -82%), bleeding or malaena (18 -29%), constipation (4 – 29%) abdominal mass (24 – 42%)
- 4 locations are typically involved usually at a junction between freely moving segments and retroperitoneally or adhesionally fixed segments
- Entero-enteric – confined to the small bowel
- colo – colic – involving the large bowel only
- ileo-colic – telescoping of the terminal ileum into the ascending colon
- ileo-cecal – the ileocecal valve is the leading point (difficult to distinguish from ileo – colic)
Investigations
- CT is the most sensitive investigation for the diagnosis of intussusception (59 -100% accuracy) CT features include
- inhomogeneous “target” or ‘sausage” shaped soft tissue mass with layering effect
- Mesenteric vessels visible within the bowel wall
- May differentiate intussusception without a lead point (no signs of proximal bowel obstruction, target -like or sausage shaped mass, layering effect) from that with a lead point (features of bowel obstruction, target like or sausage shaped mass, layering effect)
- US useful in children and adults
- ‘doughnut’ sign in the transverse view
- ‘ pseudo-kidney” or ‘hay fork’ sign in the longitudinal view
Treatment
- In adults – all require surgical treatment because of the high incidence of malignancy
- Preop manipulation is not advised in adults as this may lead to
- intraluminal seeding and venous tumour dissemination
- perforation and seeding of microorganisms and tumour cells to the peritoneal cavity
- increased risk of anastomotic complications of manipulated friable and oedematous tissue.
- In children – most intussusceptions are benign, so reduction with air contrast enemas.
Teaching point: Ultrasound should be the initial investigation for all abdominal masses in the Emergency Department. This should be done as a focussed, point of care scan where the mass is directly insonated.
References
- Open access Emerg Med: Review article Adult intussusception: a continuously unveiling clinical complex illustrating both acute (emergency) and chronic disease management. PA Ongom*, SC Kijjambu
- Case report Gastroenterol 2013 Sep 5;7(3):381-7. doi: 10.1159/000355155. eCollection 2013.
Adult colocolic intussusception and literature review. Wilson A1, Elias G, Dupiton R. - The Permanente journ :Adult Intussusception Teng Lu, MD
- Radiopaedia: Intussusception Dr Behrang Amini et al.