



Images and Text Genevieve Carbonatto
A 45 year old man presents with a 3 day history of diarrhea and increasing LIF pain. He is afebrile. His diarrhea has tapered off. On examination he is tender in his LIF. A point of care ultrasound is performed using a curvilinear probe. He is able to localise with precision his area of tenderness.
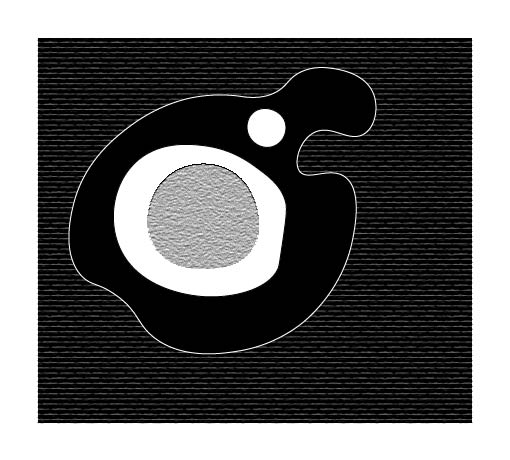
This is his scan


At his area of maximum tenderness there is a diverticulum which is clearly visible. The colon is thickened and stands out against the surrounding hyperechoic inflamed mesentery. A CT confirms the diagnosis
Discussion
Diverticulitis is a common presentation to the Emergency department. It is a herniation of the mucosa and submucosa, corresponding to a weak point where the vasa recti penetrate the tunica muscularis, so most colonic diverticula are “false diverticula” containing no muscularis propria.
Imaging technique
- Transducer : Curvilinear transducer first to “scout the area”. May change to linear high frequency transducer if the patient is slim.
- Sweep over the area of tenderness and ask the patient to put the transducer over the maximal area of tenderness.
- Identify the thickened loop of colon and assess in it’s long axis first then scan through the entire length in the short axis
- Look for :
- At least one diverticulum.
- Local thickening of the bowel wall > 4 -5 mm.
- A faecolith or air which may be visible in the inflamed wall of the colon presenting as an echogenic focus accompanied by an acoustic shadow.
- Echogenic non compressible fat surrounding one or more diverticula suggesting an acute inflammatory process.
- Identification of a “target sign” when the segment is examined in the transverse view. This refers to a thickened hyoechoic wall (the muscularis propria) of the bowel surrounding an echogenic centre.
- In the longitudinal view, look for a bowel segment which will appear tubular with narrowing or complete obstruction of the lumen.

The following images are examples of diverticulitis.
Case 1
Transverse view of the inflamed area. The hypoechoic thickened wall of the colon is visible. A diverticulum is seen and a faecolith is identiied casting an acoustic shadow.


Longitudinal view of the inflamed area. The wall is thickened, a diverticulum and faecolith are visualised. The lumen of the bowel segment is not visible.


Case 2
By scanning in the transverse axis distally along the colon, the relatively short length of colon inflammation and the diverticulum are visible. The pathology lies precisely under the area of tenderness.
Ultrasound in Diverticulitis (1)
The overall accuracy of ultrasound in prospective studies has been found to be equivalent to CT with one study showing overall accuracy of detection of diverticulitis using ultrasound of 98%. CT may be superior however in the following circumstances:
- In obese patients
- When the area of interest is obscured by gas
- When the distal sigmoid colon is involved
- In cases of complicated diverticulitis associated with free air, faecal peritonitis or deep abscesses
- When the diagnosis is not diverticulitis and an alternative diagnoses to diverticulitis such as ureterolithiasis, pyelonephritis, perforated peptic ulcer, appendicitis, Crohn’s disease, gynecological conditions, colonic malignancy, pancreatitis is the cause of the patient’s symptoms
It is possible to repeat daily ultrasounds. It has been shown that diverticulitis runs a predictable and benign course which can be followed using ultrasound. At first there is local wall thickening of the colon with preservation of the ultrasound layer structure. Within the inflamed diverticulum a fecolith is present. The diverticulum is surrounded by hypoechoic , non compressible tissue . This is followed by evacuation of the faecolith to the colonic lumen with or without the development of a small paracolic abscess, sometimes with the disintergration of the faecolith within 1 -2 days. The remaining inflammatory changes remain present for several days after the evacuation of the faecolith
Diverticulitis may be right sided (left : right 15:1) Diverticula of the right colon are usually solitary, congenital, true diverticula containing all bowel layers. The faecoliths are larger and the diverticula neck wider. There is no hypertrophy of the muscularis of the right colonic wall.
References:
- Dig Dis 2012;30:56–59 (DOI:10.1159/000336620)Ultrasound of Colon DiverticulitisPuylaert J.B.C.M
- World J Emerg Med. 2016; 7(1): 74–76. Ultrasound diagnosis of diverticulitis Michael E. Abboud, Sarah E. Frasure, and Michael B. Stone
- Clin Colon Rectal Surg. 2004 Aug; 17(3): 155–162.Diverticular DiseaseGuest Editor David E. Beck M.D. Richard E. Karulf M.D.Imaging of Colonic Diverticular Disease
Michael Jesse Snyder, M.D.1,2
Excellent teaching presentation
SIMPLE EXPLANATION WITH GOOD INFORMATIVE PRESENTATION
Thank you!
SIMPLE EXPLANATION WITH GOOD INFORMATIVE PRESENTATION
Thanks Waleed. Diverticulitis is very easy to diagnose with ultrasound and extremely helpful in a busy ED especially if you do not have CT available 24/7