



Images Micky Fiorentino
Triage:
A 46 year old lady presented to the Emergency department after being referred by the early pregnancy assessment clinic for an ectopic pregnancy and admission under O and G. She is 11 weeks pregnant. It is an IVF pregnancy. She is hemodynamically stable and is not complaining of abdominal pain.
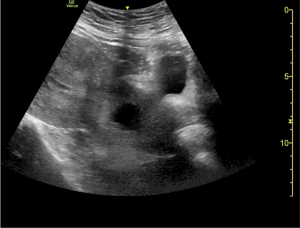
This is a sweep through her uterus in the longitudinal plane. What can you see?
The uterus is retroverted and there is a gestational sac low down in the uterus at the level of the cervix. This is a cervical ectopic pregnancy. There is what is referred to as an hourglass appearance of the uterus. The “waist ” of the hour glass is at the level of the internal os. The gestational sac has a thick echogenic rim.

How would you check for a fetal pole and a fetal heart beat?
First you would zoom onto the gestational sac and carefully sweep through it both in the longitudinal and transverse plane to look for a fetal pole. Once you have done that you would hold the probe still and look for the flicker associated with a fetal heart beat.


Once the fetal heart beat is identified you need to prove the presence of the heart beat by putting an M mode cursor through the heart.


You can then map out the heart beats and by mapping out the start of one heart beat with a cursor and the start of another 2 beats away, the machine will give you the fetal heart rate.
.

Why do we use M mode in the first trimester to identify the fetal heart beat and not Doppler?
M mode has great temporal resolution. M mode shows you the movement of echos over time with great accuracy. This is why it is used in ECHO to look at cardiac wall motion or valve motion and in early pregnancy, cardiac activity. Doppler is never used in the embryonic stage of the first trimester because Doppler uses more power output, causing more heating of the tissues. It is unclear how safe these thermal effects are on the developing fetus.
What is a cervical ectopic and how common is it?
There are many locations for ectopic pregnancies. In total ectopic pregnancies make up about 2% of all pregnancies. 95% of all ectopics are tubal. Cervical ectopic pregnancies are extremely rare , the incidence being approximately 1 in 9000 pregnancies. A cervical ectopic is when the fertilized ovum implants directly into the wall of the cervix below the level of the internal os.

How could you differentiate between a cervical ectopic and an inevitable miscarriage?
An inevitable miscarriage is when the gestational sac is being evacuated and moving down towards the cervical canal. A cervical ectopic and an exiting gestational sac may look very similar. These are the characteristics of a gestational sac in the endocervical canal from an inevitable miscarriage
- The sac is not usually round. It may be irregular, flattened or crenated border.
- The presence of a fetal pole with an active heart beat increases the likelihood of a cervical ectopic.
- Jurvonic et al describe the “sliding sign” to differentiate between the two. An aborting gestational sac will slide up and down with gentle transabdominal pressure whilst an ectopic cervical pregnancy will not
Reference:
Callen’s Ultrasonography in Obstetrics and Gynecology 6th edition