




Images Juan Chiang
A 13 year old girl presents to the Emergency Department after a syncopal event at school. This was not associated with prior chest pain or SOB. This is her first syncopal event.
ECG

Chest Xray

A point of care ultrasound is performed.
The following clip shows her PLAX view followed by her PSAX then the 4 CV and then colour Doppler through her tricuspid valve in the 4CV
PLAX
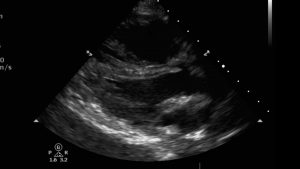

The PLAX shows a large RV, flattening of the IVS towards the LV in both systole and diastole and a small LV cavity
PSAX


The PSAX also shows a large RV and a D shaped LV due to flattening of the IVS


The 4 CV confirms the very dilated RV cavity (the RV should be 2/3 of the size of the LV normally) , the small LV cavity due to the IVS being pushed towards the LV due to the high pressures in the RV. The RA is dilated compared to the LA.

Pulmonary arterial pressures were measured at 70mmHg . She was transferred to the cardiology ward for ongoing assessment and treatment.
Discussion
The definition of pulmonary arterial hypertension is the same in children as it is in adults . It is a mean PAP of greater than 25mmHg at rest. In fetal circulation, the PAP is similar to that of the systemic circulation but after birth drops significantly to achieve levels similar to adults at 3 months of age. This definition therefore applies to children older than 3 months of age.
Pulmonary hypertension in children is multifactorial and it’s aetiology different to that of adults. Children have a greater incidence of
- idiopathic pulmonary arterial hypertension (IPAH)
- pulmonary arterial hypertension (PAH) due to congenital heart disease (PAH-CAD)
- Developmental lung disease (Brochopulmonary dysplasia (BPD), congenital diaphragmatic hernia, Down’s syndrome, lung hypoplasia
- Others (drug and toxins, portal hypertension, persistent pulmonary hypertension of the newborn, congenital post capillary obstructive lesions, haematological, systemic and metabolic disorders)
Epidemiology
- The estimated incidence of sustained pulmonary artery hypertension is around 4- 10 cases per million children per year
- The prevalence in Europe (Spain, the Netherlands) is around 20 -40 cases per million chidren
The prognosis for PAH in children is poor if left untreated. The median untreated survival for children is 10 months as apposed to 2.4 years for adults if left untreated.
Presentation
The diagnosis of PH is often delayed in children because of the non specific symptoms . The most common misdiagnosis is asthma. Clinical presentation will depend on the age of the patient, the presence or absence of associated medical conditions, the severity of the pulmonary hypertension, RV function.
Signs and symptoms include
- SOB on exertion
- fatigue
- syncope
- cyanosis (with exertion or at rest)
- failure to thrive
- cough
- chest pain
- heart failure (uncommon)
The degree of symptoms depends on on how well the RV adapts to the increased pressure. If pulmonary hypertension is present since birth, RV hypertrophy occurs and RV function is preserved. These patients may present late.
Management at time of diagnosis ( ED and cardiology)
- comprehensive history and examination
- chest xray (dilatation of proximal and main pulmonary arteries, cardiomegaly due to RV dilatation)
- FBC, UEC, BNP (BNP is used to assess severity and monitor response to therapy in children and adults with heart failure)
- ECG (right atrial enlargement – p pulmonale, RV hypertrophy – tall R waves in V1 > 20 mm, deep S waves in V5, V6, R axis deviation, ST -T wave abnormalitie in inferior leads
- ECHO ( for functional and structural assessment. TAPSE – tricuspid annular plane systolic excusion, has been strongly associatde with improved survival during treatment)
- chest CT with or without contrast to assess for underlying lung disease
- 6 minute walking test
- Right and left catheterisation for diagnosis and to direct therapy. Measurement of systolic, mean, and diastolic systemic arterial, RA , RV systolic and end diastolic pressures and systolic, mean and diastolic PAPs, including bilateral pulmonary arterial wedge pressures. Acute vasoreactivity testing (VRT) to assess prognosis and indication for specific PH therapy. This involves administering vasoactive drugs such as nitric oxide , aerosoled iloprost to look for any change in mean pulmonary artery pressure. If vasoactive testing is positive then calcium channel blockers are indicated
- idiopathic pulmonary hypertension is a diagnosis of exclusion due the diverse aetiology of pulmonary hypertension
Ongoing management
- Treat underlying cause if possible
- Regular follow up at pulmonary hypertension clinic every 3 -6 months
- Immunisations need to be up to date including pneumococcal and yearly influenza vaccines. RSV immunoprophylaxis is important
- Early treatment of respiratory illnesses
- Antibiotic prophylaxis for prevention of bacterial endocarditis in patients when appropriate for cyanotic patients and patients with CHD
- Strenuous exercise needs to be avoided
- Supplementary oxygen during airplane flights
- Selected drug therapies include
- warfarin has shown improved survival INR 1.5 – 2.5
- calcium channel blockers if VRT positive
- pulmonary artery specific vasodilators such as prostocyclin analogues (esoprostenol), endolethin receptor antagonists (bosentan) and phosphodiesterase type 5 inhibitors (sildenafil, tadalafil)
- oxygen
- diuretics
9. Surgery
- atrial septostomy has been used as a bridge to lung transplant and has been been found to improve the quality of life in paediatric patients with PAH who are no longer responsive to medical therapy
- lung transplant